- BACKGROUND
-
 THYROID
THYROID
-
 PARATHYROID
PARATHYROID
-
 ADRENAL
ADRENAL
-
 OBESITY
OBESITY
-
 DIABETES
DIABETES
-
 PANCREAS
PANCREAS
-
 PITUITARY
PITUITARY
-
 THYMUS
THYMUS
-
 BREAST
BREAST
-
 DIABETIC FOOT
DIABETIC FOOT
-
 RARE TUMOURS
RARE TUMOURS
BACKGROUND
Endocrine science is a unique division within the vast medical science and human biology. Almost all the activities such as muscle contraction, respiration, circulation, heart, brain, kidney, bone functions are mediated through a multitude of hormones and chemical factors secreted by seven major and several minor endocrine glands distributed from head to toe of the human body. Majority of the body functions need appropriate levels of these hormones circulating in blood. Any increase or decrease in the hormone levels lead to disturbance in these activities leading to suffering on part of the patient in the form of several symptoms. These symptoms can range widely from weight gain/ loss; change in apetite, weakness, muscle pain, headache, increase in heart rate, disturbance in menstrual cycles etc., In addition the major endocrine glands such as thyroid, pituitary, parathyroid, pancreas, adrenal glands can be affected with tumours and cancers leading to local pressure symptoms and above hormonal disturbances.
Endocrine diseases such as hypothyroidism, hyperthyroidism, goiters; diabetes; obesity; metabolic bone disease are very common conditions in the society affecting at least 1 out of 30 people. Some diseases such as congenital hypothyroidism, lingual thyroid are common in children and hashimotos thyroiditis and goiters in adults and diabetes in elderly. Most of endocrine diseases such as diabetes, obesity, vitamin D deficiency are modern day epidemics and life style related due to fast food culture and working in confined air-conditioned environments. Though adrenal, pituitary and endocrine disorders are less common compared to thyroid and diabetes occurring in 1 out of 1000 individuals in society. One of the causes for rarity of adrenal, pancreatic disorders is lack of awareness amongst physicians, general practitioners missing the cases. In effect, patients suffer for years together with the disorders such as pheochromocytoma, cushings syndrome, insulinoma, prolactinoma and often die with the disorders undiagnosed. A dedicated team of endocrinologists can diagnose these difficult endocrine diseases early and alleviate the patients suffering by tendering early optimal treatment.
The exact diagnosis of underlying syndrome and optimal treatment is one of the greatest fascinating challenges in entire medical field.
Four essential steps in long term for any endocrine disease are:
- Suspicion (suspecting the disease) based on patients symptoms
- Clinical examination
- Hormonal testing
- Appropriate imaging
Four essential steps in the treatment of any endocrine disease are:
- Confirmation of diagnosis
- Counseling patient regarding their disease
- Medical treatment
- Surgical treatment after preoperative preparation (if surgery is needed)
Four essential steps in long term for any endocrine disease are:
- Life long follow-up
- Periodical testing and monitoring
- Early detection of any exacerbation or recurrence of disease
- Screening of family members (in certain syndromes)
All these aspects of patient care is dynamic and varies from patient to patient. This whole process requires highly knowledgeable experts, specialists and it is a team work. It is not a single man army. For optimal results, comprehensive multidisciplinary approach with appropriate intervention at strategic time frame taking patient in to confidence and educating them about their disease is vital. We offer hormonal therapy, surgical treatment for endocrine tumours, radio-iodine treatment for thyroid cancer depending on the patients need.
THYROID

The thyroid gland is a butterfly shaped 20 – 25 grams gland situated in front of neck beneath the skin and in front of windpipe. It releases a very important hormone called thyroxine in to our blood at a constant rate daily. With this hormone it controls all the functions of body organs such as heart, brain, lung, muscles, bone, blood, liver, kidney, eyes etc., Both increased levels of hormone (hyperthyroidism) and decreased levels of hormone (hypothyroidism) causes lot of symptoms and disturbances in body functions. Apart from that even cancer and nodules can occur in thyroid gland.
The common symptoms of thyroid include :
- Graves' disease
- Multinodular goiter, other nodules
- Hashimoto's thyroiditis
- Thyroid cancer
- Hypothyroidism
- Dyshormonogenetic goiter
The common surgeries performed for thyroid disease are:
- Hemithyroidectomy (where half of gland is removed)
- Total thyroidectomy (whole of the gland is removed)
- Sternotomy and thoracotomy (Chest is opened for large gotier extending outside neck)
- Thyroidectomy with Lymph node dissection (for thyroid cancer)
- Endoscopic thyroidectomy (for scarless neck)
SUGGESTED REFERENCES:
- Bhargav PRK, Mishra A, Agarwal G, Agarwal A, Verma AK, Mishra SK. Clinicopathological profile and long term outcome of differentiated thyroid cancer – Experience from a developing country. World J Surg. 2010 Jan;34(1):40-7
- Bhargav PRK, Mishra A, Agarwal G, Agarwal A, Verma AK, Mishra SK. Prevalence of hypothyroidism in benign breast disease and outcome of thyroid hormone replacement therapy. World J Surg. 2009 Oct;33(10):2087-93
- Bhargav PRK, Amar V, Kishan rao, Murthy SGK, Gayathri KB. CAVATT (Combined Cervical and video-assisted thoracoscopic thyroidectomy: A simplified and innovative approach for posterior mediastinal goiter. Indian J Surgery 2010;72 (4):336
- Bhargav PRK, Gayathri KB. Synchronous occurrence of anaplastic, follicular and papillary carcinomas with follicular adenoma in thyroid gland 2011;54(2):414-5
- Bhargav PRK, Kusumanjali A, Nagaraju R, Amar V. What is the Ideal CO2 Insufflation Pressure for Endoscopic Thyroidectomy? Personal Experience with Five Cases of Goiter. World J Endocrine Surg. 2011;3(1):3-6
- Bhargav PRK, Amar V, Venkata Pavan Kumar CH, Gayathri KB. Pipestem Carotids as a marker of vascular insult in Graves' disease. Indian J Surgery 2010;73(2): 168-169
PARATHYROID
Parathyroid glands are four in number and very small (< 1 cm) glands situated on the back side of thyroid gland in neck. Parathyroid glands secrete parathyroid hormone (PTH) and are vital for maintaining calcium levels in body and thereby proper function of muscle, bone, brain, heart and gut. Excess hormone results in high levels of serum calcium and low levels result in hypocalcemia.
If a tumour or any other disease causes increased release of PTH it increases blood calcium levels (Hypercalcemia) and the condition is called Hyperparathyroidism (HPT) and decreased levels of hormone leads to decreased calcium levels (Hypocalcemia) and the condition is called hypoparathyroidism. Both are dangerous conditions if not properly treated. There are several causes and diseases affecting parathyroid glands and body calcium levels.
- Primary hyperparathyroidism (PHPT) – due to parathyroid tumour (adenoma) or cancer
- Secondary hyperparathyroidism (SHPT) – due to renal disease or vitamin D deficiency
- Teritiary hyperparathyroidism (THPT) – renal and bone disease
- Hypoparathyroidism – infections and metabolic diseases
Primary hyperparathyroidism (PHPT) :
- Renal stones related – pain, infection etc.
- Bone problems – pain, fractures, swellings etc.
- Muscle weakness – unable to comb hair, getting up after squatting etc.
- Gastritis – hyperacidity
- Mood disturbances – memory loss, depression, emotional lability etc.
- Hypertension. These classical features are called famously as " BONES, STONES, GROANS, MOANS, OVERTONES" in medical field.
Frequent surgeries done for parathyroid disease are:
- Open neck surgery – Bilateral standard neck exploration
- Focussed parathyroidectomy
- Endoscopic parathyroidectomy
- Radio-immuno guided surgery
- Unilateral parathyroidectomy
- Parathyroid autotransplantation
The choice of these operations depends on several factors such as patient disease type, size of gland. associated other diseases and best adjudged by an experienced endocrine surgeon after discussing with patient and attendant after thorough clinical evaluation and investigations.
SUGGESTED REFERENCES:
- Bhargav PRK. Role and feasibility of IOPTH in guiding parathyroid surgery. Accepted in Indian J Surg. 2013
- Bhargav PRK. Salient Anatomical Landmarks of thyroid and their practical significance in Thyroid Surgery: A Pictoral review of Thyroid surgical anatomy (Re-visited). Indian J Surg. 2013 DOI: 10.1007/s12262-013-0856-x
- Aggarwal V,Bhargav PRK, Mishra A. Giant parathyroid adenoma. ANZ J Surg. 2009 Jan-Feb;79(1-2):91
ADRENAL
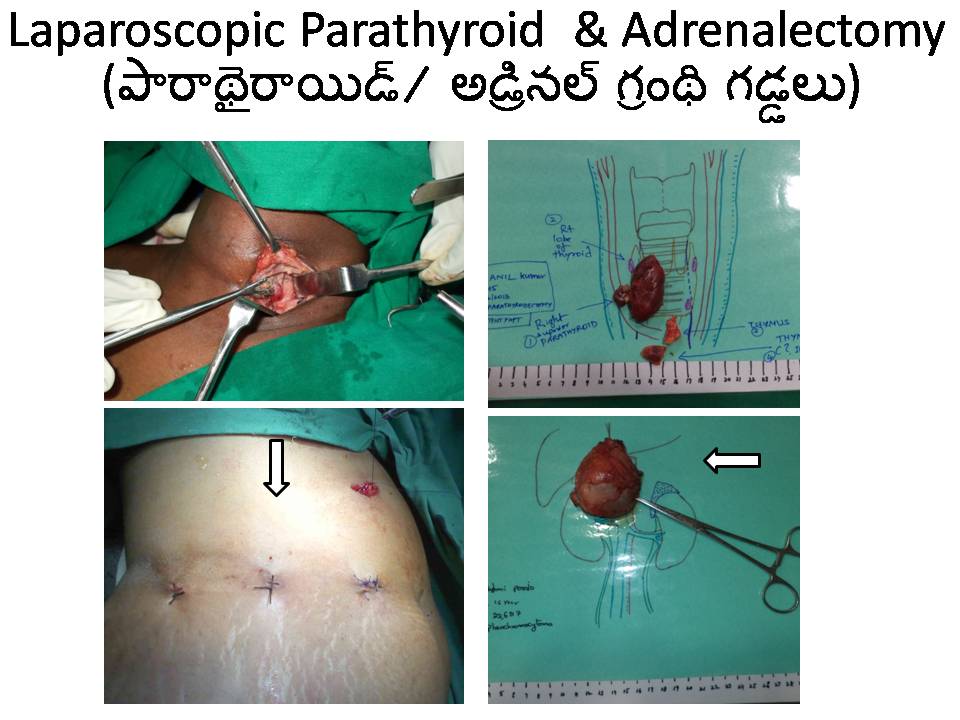
There are two roughly triangular shaped adrenal glands one on each kidney in our tummy. Adrenal gland is vital for maintainence of human life as it secretes many essential hormones with multiple functions in our body. The outer part called Cortex releases glucocorticoid, mineralocorticoid and sex hormones. The inner part called as Medulla releases epinephrine and nor-epinephrine hormones.
Coritcosteroids maintain our immunity and functions in mediating integrity of tissues and metabolism. Mineralocorticoids help in maintaining blood pressure, salt and water balance of our body. Sex steroids help maintain sexual function and fertility in both men and women. Medullary hormones help in maintaining blood pressure.
Increased release of any of these hormones occurs due to a variety of tumours or cancers and cause multiple problems such as hypertension, diabetes, infections, bone pains, osteoporosis, blindness, water and electrolyte imbalances etc., Decreased release of hormones occurs in a condition called Hypoadrenalism or Addison's disease.
The common tumours of Adrenal gland are:
- Aldosteronoma (Conn's syndrome)
- Cushing's syndrome.
- Pheochromocytoma.
- Adrenocortical cancer.
- Addison's disease.
- Cysts, Myelolipomas.
- Fungal infections, tuberculosis.
- Secondary metastases.
- Congenital adrenal hyperplasia
Treatment :
The treatment of any adrenal disease is a complex issue, and includes medical hormonal treatment, control of infections, heart function, blood pressure, muscle power followed by surgery in indicated patients. Surgical removal of adrenal gland is called Adrenalectomy. It can be done either by open approach or laparoscopy. It needs high degree of expertise and experience. It is a major operation which requires knowledge on part of endocrine surgeon of anaesthesia. In expert hands it is a straight forward operation with least complications. Adrenal cancers need radiotherapy and/ or chemotherapy. After operation patient may require to take hormonal replacement for a brief period of 6 months to 1 year.
The common indications for Adrenalectomy are:
- Cushing's adenoma
- Aldosteronoma
- Pheochromocytoma
- Incidentaloma
- Failed pituitary surgery in Cushing's disease
SUGGESTED REFERENCES:
- Bhargav PRK, Mishra A, Agarwal A, Agarwal G, Verma AK, Mishra SK. Adrenal Incidentalomas – Experience in a developing country. World J Surg. 2008 Aug;32(8):1802-8
- Bhargav PRK, Pradeep PV, Mishra A. Clinical and biological features in the prognosis of Adrenocortical Cancer: Poor outcome of cortisol secreting tumors in a series of 202 consecutive patients. J Clin Endocrinol Metab 2006; 91: 2650-2655
- Pradeep PV, Mishra A K, Agarwal V , Bhargav PRK , Gupta SK , Agarwal A. Adrenal cysts: an institutional experience: World J Surgery 2006, Vol 30 No: 10; 1817-1820
OBESITY

It has become a major public health problem in most of the countries including developing ones. Altered life style and certain genetic events has forged this epidemic into serious proportions to the extent of 30 % in some nations. If not corrected it leads to numerous health hazards such as diabetes, hypertension, arthritis, hyperlipidemia, cardiac, renal, liver problems, infertility etc., Several classifications and definitions for degrees of obesity are proposed, but the most widely accepted classifications are those from the World Health Organization (WHO), based on body mass index (BMI).
The WHO designations are as follows:
- Grade 1 overweight (commonly and simply called overweight) - BMI of 25-29.9 kg/m2
- Grade 2 overweight (commonly called obesity) - BMI of 30-39.9 kg/m2
- Grade 3 overweight (commonly called severe or morbid obesity) - BMI ≥40 kg/m2
Treatment:
-
Treatment of obesity starts with comprehensive lifestyle management (ie, diet, physical activity, behavior modification).
The 3 major phases of any successful weight-loss program are as follows:
- Screening phase
- Weight-loss phase
- Maintenance phase - This can conceivably last for the rest of the patient's life but ideally lasts for at least 1 year after the weight-loss program has been completed
Medications:
-
Currently, the 3 major groups of drugs used to manage obesity are as follows:
- Centrally acting medications that impair dietary intake
- Medications that act peripherally to impair dietary absorption
- Medications that increase energy expenditure
Surgery:
Surgery has emerged as the most effective option with significant weight loss and correction of abnormalities like diabetes, hypertension, arthritis, hyperlipidemia, infertility etc., It causes sustained weight loss in selected patients. The surgery for reversal of obesity is called Bariatric surgery and those done for correction of metabolic abnormalities such as diabetes or hyperlipidemia is called Metabolic Surgery
-
Among the standard bariatric procedures are the following:
- Roux-en-Y gastric bypass.
- Adjustable gastric banding.
- Gastric sleeve surgery.
- Vertical sleeve gastrectomy.
- Horizontal gastroplasty.
- Vertical-banded gastroplasty.
- Duodenal-switch procedures.
- Biliopancreatic bypass.
- Biliopancreatic diversion.
DIABETES
Diabetes mellitus is an epidemic and afflicts population of countries worldwide. Diabetes mellitus consists of an array of dysfunctions characterized by hyperglycemia and resulting from the combination of resistance to insulin action, inadequate insulin secretion, and excessive or inappropriate glucagon secretion.
-
Many patients with type 2 diabetes are asymptomatic. Clinical symptoms include the following:
- Classic symptoms: Polyuria, polydipsia, polyphagia, and weight loss.
- Blurred vision.
- Lower-extremity paresthesias.
- Fungal infections
Diagnostic criteria by the American Diabetes Association (ADA) include:
- A fasting plasma glucose (FPG) level of 126 mg/dL (7.0 mmol/L) or higher
- A 2-hour plasma glucose level of 200 mg/dL (11.1 mmol/L) or higher during a 75-g oral glucose tolerance test (OGTT)
- A random plasma glucose of 200 mg/dL (11.1 mmol/L) or higher in a patient with classic symptoms of hyperglycemia or hyperglycemic crisis
Treatment:
-
Diabetes treatment is a multi-disciplinary and lifelong issue. Management includes the following:
- Appropriate goal for glucose levels.
- Dietary and exercise modifications.
- Medications.
- Appropriate self-monitoring of blood glucose (SMBG).
- Regular monitoring for complications.
Medications used in diabetic therapy include the following:
- Sulfonylureas.
- Meglitinide derivatives.
- Alpha-glucosidase inhibitors.
- Thiazolidinediones (TZDs).
- Glucagonlike peptide–1 (GLP-1) agonists.
- Dipeptidyl peptidase IV (DPP-4) Inhibitors.
- Selective sodium-glucose transporter-2 (SGLT-2) inhibitors.
- Insulins.
- Amylinomimetics.
- Bile acid sequestrants.
- Dopamine agonists.
PANCREAS
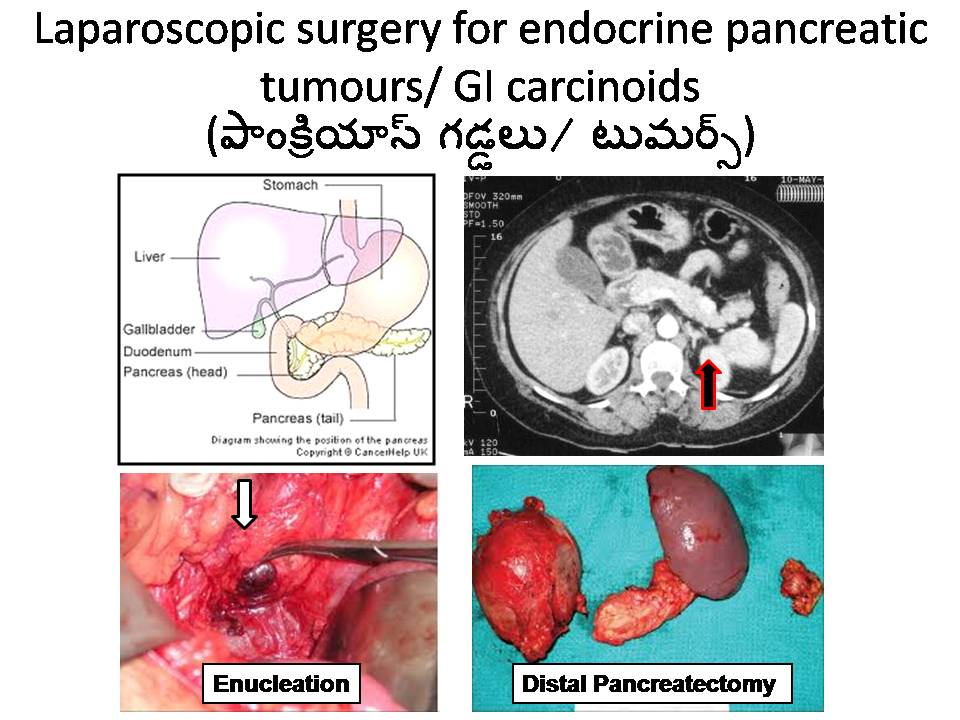
Pancreas gland is a special type of gland located on the back side of stomach and contains an largest exocrine part and smaller endocrine part. Exocrine part secretes enzymes for digestion of fat. Endocrine part is formed by Islets of Langerhans and consists of special cells called alpha, beta, delta and PP cells. Each cell secretes its own special hormone vital for the function of glucose metabolism, maintaining acidity of stomach and digestive functions. Rarely, tumours and cancers involving these cells can occur which needs expert medical and surgical treatment
The cells – hormone secreted and respective tumours are -
- B cells – Insulin – Insulinoma.
- A cells – Glucagon – Glucagonoma.
- G cells – Gastrin – Gastrinoma.
- D cells – Somatostatin - Somatostatinoma.
- VIP - VIP - VIP oma.
These tumours and neoplasms usually occur in 30 – 50 years age group. Symptoms of these tumours widely vary and can involve any body function depending on tumour type.
For example:
- Insulinoma – hypoglycemia manifested by fainting attacks, weight gain etc.
- Gastrinoma – hyperacidity, diarrhea, peptic ulcers etc.
- VIPoma – diarrhea, hypokalemia, diabetes etc.
- Glucagonoma – diabetes, diarrhea, weight loss.
PITUITARY
The pituitary gland is small pea-sized endocrine gland located at the base of the brain beneath the hypothalamus. It is often regarded as the most important gland amongst all other endocrine glands as it secretes hormones which can control all other endocrine glands famously known as "MASTER OF ENDOCRINE ORCHESTRA".
-
The pituitary gland is divided has two parts: the anterior lobe and the posterior lobe. The anterior lobe produces the following hormones, which are regulated by the hypothalamus:
- Growth hormone: Stimulates growth of bone and tissue (growth hormone deficiency in children results in growth failure. Growth hormone deficiency in adults results stunted growth, obesity and also leads to psychological disturbances. Excess GH leads to a condition called "Acromegaly" caused by a Pituitary adenoma or tumour
- Thyroid-stimulating hormone (TSH): Stimulates the thyroid gland to produce thyroid hormones.
- Adrenocorticotropic hormone (ACTH): Stimulates the adrenal gland to produce several related steroid hormones. A pituitary adenoma leading to excess ACTH secretion causes "Cushing's disease"
- Luteinizing hormone (LH) and follicle-stimulating hormone (FSH): Hormones that control sexual function and production of the sex steroids, estrogen and progesterone in females or testosterone in males
- Prolactin: Hormone that stimulates milk production in females
The posterior lobe releases the following hormones, which are not regulated by the hypothalamus:
- Antidiuretic hormone (vasopressin): Controls water loss by the kidneys
- Oxytocin: Contracts the uterus during childbirth and stimulates milk production
Treatment of disease:
A pituitary adenoma can be of variable sizes. A < 1 cm adenoma is called microadenoma, which is amenable to medical and surgical treatment. A > 1 cm tumour is called macroadenoma, which can lead to local pressure effects like diplopia, cavernous sinus thrombosis, hypopituitarism etc.
The commonest surgical treatment offered for pituitary adenomas are:
- Trans-sphenoidal microadenectomy (Done endoscopically through nose and sphenoid sinus)
- Trans-sphenoidal hypophysectomy
- Total hypophysectomy
- Trans-cranial surgery (Done through skull opening for large invasive tumours)
- For inoperable cases, Radiotherapy may be chosen
THYMUS

The thymus gland is a roughly 'H' shaped gland located in upper part of chest infront of heart and just below the neck. It has vital function of priming the immune system before 20 years of age. After that it is largely a vestigial organ and undergoes gradual atrophy by 50 year of age due to fibrosis. Though it has limited function normally, it can be seat for many diseases.
- In myasthenia gravis, it undergoes hyperplasia and removal of it (Thymectomy) corrects it in atleast 30 – 40 %.
- Tumours and cancers can occur in thymus rarely.
- Thymic carcinoid, an endocrine surgical condition, in which many different ectopic hormones can be secreted leading to Syndromes. Eg., Cushing's syndrome, Pheochromocytoma etc.
- Thymus gland can be seat for Ectopic thyroid gland and related goiter.
- Thymus gland can be seat for ectopic parathyroid gland.
Treatment of disease:
Surgical removal of thymus is called THYMECTOMY. It can be done through 1) Neck (cervical); 2) Chest front (Sternotomy); 3) lateral chest (Thoracotomy); 4) Endoscopic (Thoracoscopy)
Perioperative care: The essential steps for success of treatment and thymectomy are :
- Exact diagnosis.
- Imaging – CT scan; MRI.
- Hormonal evaluation.
- Preoperative preparation especially chest.
- Optimisation of disease condition and co-morbidities with medications.
- Meticulous postoperative care (ICU support).
- Chest physiotherapy.
- Long term (life long followup).
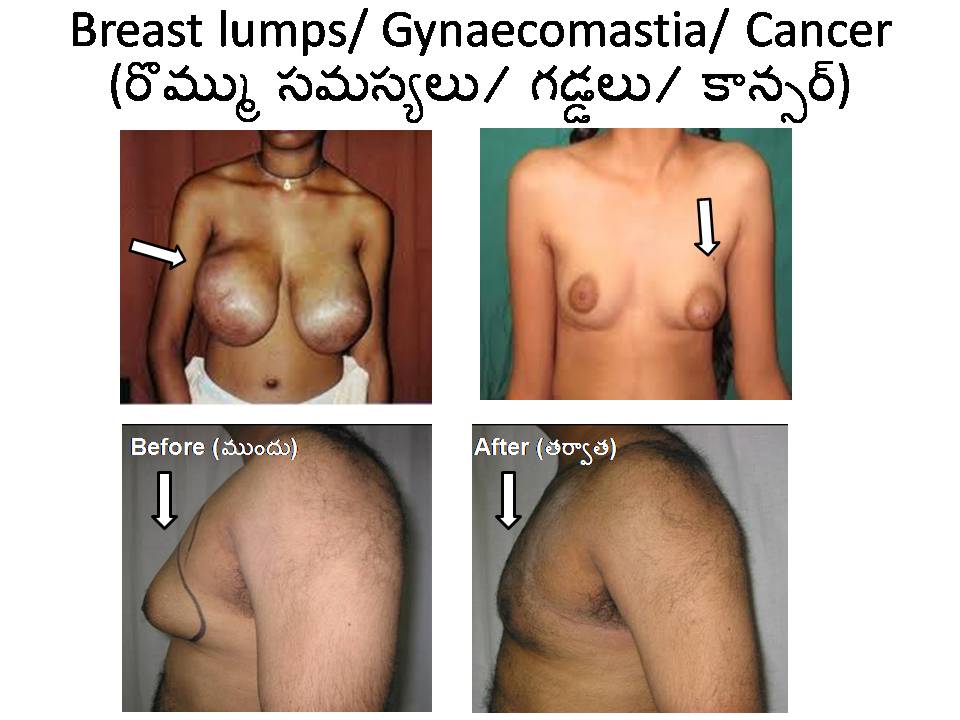
BREASTS
Though breasts perse is not an endocrine gland but many hormonal related diseases occur in breasts requiring endocrine treatment.
The common diseases include:
- Gynaecomastia (in males).
- Benign breast disease – fibroadenoma, cyst.
- Nipple discharge.
- Breast cancer.
DIABETIC FOOT
Diabetes is a disease syndrome characterized by high blood glucose levels and over time can damage the nerves, kidneys, eyes, and blood vessels. By compromising immunity, diabetes can also decrease the body's ability to fight infection. When diabetes is not well controlled, damage to the organs and impairment of the immune system is likely. Foot problems commonly develop in people with diabetes and can quickly become serious.
- People with diabetes must be fully aware and vigilant about recognizing the foot problems as early as possible. The prevention of foot infections, ulcer and gangrene depends on a very good sugar control, nutrition, neurologic and vascular functions.
- People with diabetes should learn how to examine their own feet and how to recognize the early signs and symptoms of diabetic foot problems.
- They should also learn what is reasonable to manage routine at home foot care, how to recognize when to call the doctor, and how to recognize when a problem has become serious enough to seek emergency treatment.
RARE TUMOURS
Several rare endocrine tumours can occur throughout the body apart from aforementioned thyroid, parathyroid, adrenal, obesity, diabetes etc.,
- Tumour induced osteomalacia (a bone weakening musculoskeletal tumour).
- Carcinoid tumours in stomach, intestine, pancreas, lungs etc.
- Pineal gland tumours.
- Ectopic tumours.
- Paraneoplastic syndromes.
- Thymic carcinoids.